

Dental caries (tooth decay) is the most prevalent chronic disease worldwide, and it’s largely preventable. The earlier caries are detected the better, and BlueCheck® makes this simple.
Over 90% of people worldwide are affected by tooth decay.
The yearly cost is estimated at 2.7 million life years lost annually, and the yearly economic cost is around $300 billion.
Although there’s been an overall downward trend in caries for most Americans, that has recently reversed in young children. US Department of Health and Human Service notes "although cavities are largely preventable, they are one of the most chronic common conditions throughout the lifespan."
WHO Oral Health Report (1)
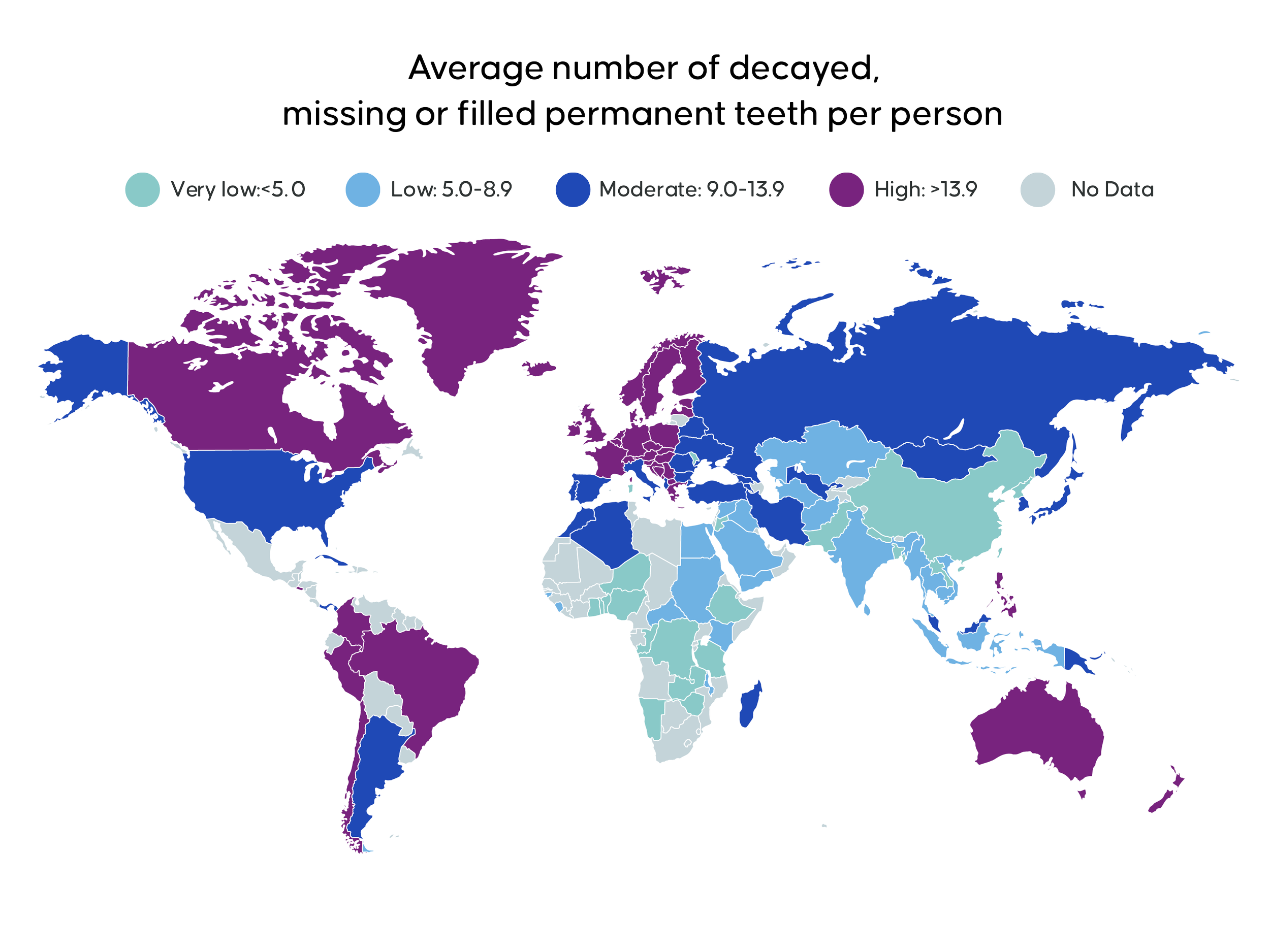
United States statistics



The WHO states that primary prevention remains the number one tool in oral health, as most oral conditions are preventable.
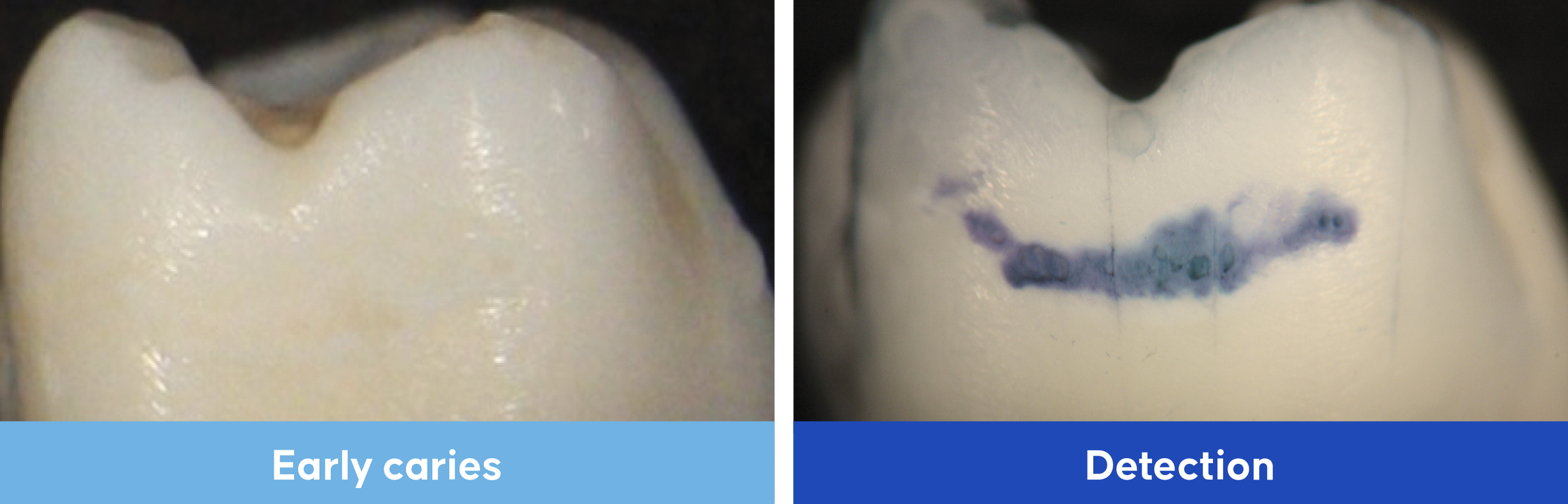
The first step in finding signs of disease is through caries detection. Current methods have limits in their ability to detect early-stage caries in enamel, these pre-visible caries are where disease begins and can be regressed by rebalancing the remineralisation process.
Mineralization and the caries process
The surface of a tooth is like a microscopic honeycomb structure of mineral crystals built into a tightly packed matrix of hydroxyapatite. There is a dynamic balance between pathological factors leading to demineralisation and protective factors supporting remineralisation of the crystalline structure and this occurs naturally throughout the day. The caries process is a continuum and which side of the balance determines whether caries form and if they progress or regress.
Our teeth decay when there is an imbalance between demineralization and remineralization. Bacteria in plaque metabolize sugars producing acid, this dissolves the crystal structure of tooth enamel (demineralization). Saliva reverses this naturally (remineralization) by supplying calcium and phosphate (in presence of fluoride) to the tooth, helping neutralize plaque acid. Remineralization treatments can also help restore the balance.

The key to arresting caries – early detection
Pre-visible lesions respond well to prevention interventions, the problem is they’re invisible – what can’t be seen doesn’t get fixed. Conversely, visible lesions that are readily detected, require more invasive treatments.

Early detection is challenging –BlueCheck makes it simple
BlueCheck makes caries lesions visible before they can be seen by the naked eye or in an radiograph, by highlighting porous areas through a distinct blue color, giving clinicians and patients clear, objective evidence of the sites of demineralization. It is a simple and cost-effective way of identifying active, early caries lesions.

Meier T et al. (2017) Global Burden of Sugar-Related Dental Diseases in 168 Countries and Health Care Costs. J Dent Res 96:845.
https://www.cdc.gov/nchs/fastats/dental.htm
U.S. Department of Health and Human Services. (2000) Oral Health in America: A Report of the Surgeon General. National Institute of Dental and Craniofacial Research, National Institutes of Health. Rockville, MD.
Centers for Disease Control and Prevention. (2019) Oral Health Surveillance Report: Trends in Dental Caries and Sealants, Tooth Retention, and Edentulism, United States, 1999–2004 to 2011–2016. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services.
Selwitz R et al. (2007) Dental Caries. The Lancet 369: 51-59.
Pretty I et al. (2006) Caries detection and diagnosis: Novel technologies. J of Dent 34:727-739.
Carr G, Murgel C. (2004) The use of operating microscopes in endodontics. Dent Clin N Am. 54:191-214.
Featherstone J. (2004) The Continuum of Dental Caries – Evidence for a Dynamic Disease Process. J Dent Res 83(Spec Iss C):39-42.
Pitts, N et al. (2017) Dental caries. Nat Rev Dis Prim, 3. 17030.
Slayton, R et al. (2018) Evidence-based clinical practice guideline on nonrestorative treatments for carious lesions JADA 149(10):837-849.
Dhar V, et al. (2023) Evidence-based clinical practice guideline on restorative treatments for caries lesions: A report from the American Dental Association. J Am Dent Assoc. Jul;154(7):551-566.
CareQuest Institute for Oral Health. (2023) The Non-Invasive Caries Therapy Guide. Boston, MA.
Mangum J et al. (2010) Surface Integrity Governs the Proteome of Hypomineralized Enamel. J Dent Res 89(10):1160-1065.